SNOMED-CT - excitement and misery
I’m trying to familiarize myself with SNOMED-CT, one of the most widely used ontologies/dictionaries for structuring clinical observations and diseases. I am focusing on this because the other popular ontology, ICD10, really didn’t deal with low level signs and symptoms that are found in clinical “History and Physical” documents. Understandable since ICD10 is focused on billing and statistical reporting to regulatory agencies.
I also concluded that it is much better to get SNOMED-CT by downloading and installing UMLS from NLM, than by downloading SNOMED-CT from the source organization, “http://www.snomed.org/” or “https://confluence.ihtsdotools.org/”. The reasons are:
-
UMLS has one file structure to hold a bunch of key ontologies I will need like RxNorm for medications, LOINC for lab tests, CPT for procedures, etc. This means I can learn one set of file formats for all
-
snomed.org did some annoying things like separated the concept code into one file and the primary text description of the code into a different file. They also included the entire history of the ontology, including obsolete terms, in the same file, whereas UMLS has a tool “Metamorphosys” that lets you keep only the active terms.
Now I’ve downloaded the SNOMED-CT files, and I’m using built-in software “Metamorphosys” to browse the terms in tree format, using their own indexes, and before loading it into any database. This software works on Windows, Mac or Linux.
The “Misery” came first. I was looking for something simple like hearing “rales” or “rhonchi” when listening to the lungs with a stethoscope. As I remember, “rales” was a term for the sounds of crackles, that represented fluid in the lowest level lung alveoli, associated with pneumoni. “Rhonchi” was a coarser sound associated with obstruction or mucous in the higher airways, associated with bronchitis. ICD10 does not have a code for either one of these.
So I walked down the tree:
- Observable Entity
- -> Clinical History Examination Observable
- -> Respiratory Observable
- -> Respiratory Characteristics of the chest
- -> Chest auscultation feature [meaning listening with a stethoscope to the chest]
Here is what I found:
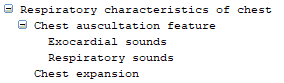
Nothing more; just synonyms for those phrases. No rhonchi or rales.
Then came the exitement! I walked down the tree on a different path:
- Clinical findings
- -> Clinical History and Observation Findings
- -> Respiratory auscultation findings
- -> Added respiratory sounds
And here is what I found below that:
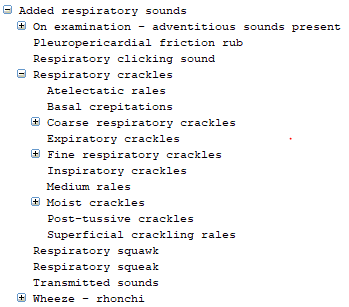
These are the little details they taught us in school, using the language they used and that we can find in a physical exam document.
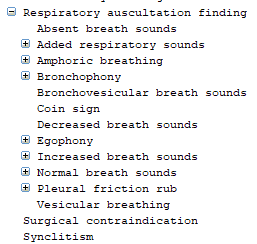
If I go further down the sub-tree “Respiratory Auscultation finding”, I get even more specialized language that I have never heard of, such as “Coin Sign”. I may never see that in a clinical document, but it’s great to know that if I do see it, this ontology will have a slot for it.
Now the trick is to find a way to detect these finely detailed clinical observations in the clinical note. My hope/belief is that this is where the gold is. If we are ever going to discover new medical knowledge, it will require looking at our medical record data at this level of detail to find new clusters and associations of observations and treatments with outcomes.
At some point, it may be better to let the model decide whether these words, in context, are important features, but SNOMED represents a way to initially focus on what many subject matter experts have designated as “atomic” features that are likely to be significant to them.